
Colorectal cancer used to be considered a disease of older people. That is no longer the case. Over the last two decades, the incidence of colorectal cancer in adults under the age of 50 has risen alarmingly. According to recent data from the American Cancer Society, incidence rates in this group have risen by almost 3% annually between 2013 and 2022 in the United States. Today, colorectal cancer is the third leading cause of cancer death in both men and women in the US, and more and more young patients are receiving this diagnosis unexpectedly.
If you or a loved one has just been diagnosed with colon or rectal cancer, we understand how overwhelming it can feel. Questions pile up quickly: What stage is it? Do I need surgery? How much will it cost? Can I continue working during treatment?
And there is one question you may not have asked yourself but should: are there treatment options outside the US that are safe, effective and significantly more affordable?La respuesta es sí. En países como Colombia, hospitales con acreditación internacional y cirujanos oncológicos formados en las mejores instituciones del mundo realizan colectomías laparoscópicas, cirugías robóticas, quimioterapia y radioterapia con los mismos protocolos utilizados en los principales centros de cáncer de Estados Unidos — a un costo entre un 50% y un 70% menor.
This guide provides you with all the information you need to assess this option clearly. We won’t pressure you or make decisions for you. Our aim is to provide you with the facts, comparisons and transparency you need to choose what’s best for your health and your circumstances.
This guide is for information purposes only and is not a substitute for professional medical advice. Always consult your oncologist or gastroenterologist before making any decisions about your treatment.
Types of colorectal cancer and treatable stages in Latin America
Understanding your diagnosis is the first step towards making an informed decision about your colorectal cancer treatment abroad. Not all colon cancers are the same, and each type responds differently to the available treatments.
Types of colorectal cancer
Adenocarcinoma: Accounts for approximately 95% of all colorectal cancers. It originates in the glandular cells that line the inside of the colon and rectum. It is the type for which there is the most scientific evidence and the widest range of treatment options. When we refer to colorectal cancer in this guide, we are primarily referring to adenocarcinoma.
Mucinous adenocarcinoma: A variant of adenocarcinoma characterised by abundant production of extracellular mucin (≥50% of tumour volume). It accounts for approximately 10–15% of cases of colorectal cancer. It is usually associated with a proximal location in the colon, a higher frequency of microsatellite instability and, in some studies, differences in clinical behaviour and response to standard chemotherapy, although results vary between series.
Carcinoid tumours: These are much less common. They arise from the neuroendocrine cells of the intestine and generally grow more slowly than adenocarcinoma. Their treatment and prognosis differ significantly.
Gastrointestinal stromal tumours (GISTs): These are rare tumours that originate in the connective tissue cells of the colon wall. They require a specialised therapeutic approach, including targeted molecular therapies such as imatinib.
Colorectal lymphoma: Extremely rare. It originates in the lymphatic tissue of the colon and requires specific oncohaematological management.
Stages of colorectal cancer (staging)
The stage of your cancer is the most decisive factor in determining your treatment plan and whether you are eligible to receive treatment in Latin America.
Stage 0 (Carcinoma in situ): The abnormal cells are found only in the innermost layer (mucosa) of the colon or rectum. They have not invaded the deeper tissue. This is usually treated by polypectomy during a colonoscopy, without the need for major surgery.
Stage I: The cancer has grown through the mucosa into the submucosa or the muscular layer of the colon wall, but has not spread to the lymph nodes or distant organs. Excellent prognosis with surgery alone.
Stage II: The tumour has penetrated all layers of the colon wall and may have spread to nearby tissues, but there is no involvement of the lymph nodes. It is subdivided into IIA, IIB and IIC according to the depth of penetration. The main treatment is surgery, with adjuvant chemotherapy in selected high-risk cases.
Stage III: The cancer has spread to nearby lymph nodes, but not to distant organs. It is subdivided into IIIA, IIIB and IIIC. It requires surgery followed by adjuvant chemotherapy. In rectal cancer, this may include neoadjuvant radiotherapy (before surgery).
Stage IV: The cancer has spread (metastasised) to distant organs such as the liver, lungs or peritoneum. It is subdivided into IVA (one organ), IVB (more than one organ) and IVC (peritoneum).
Who is eligible for treatment in Latin America?
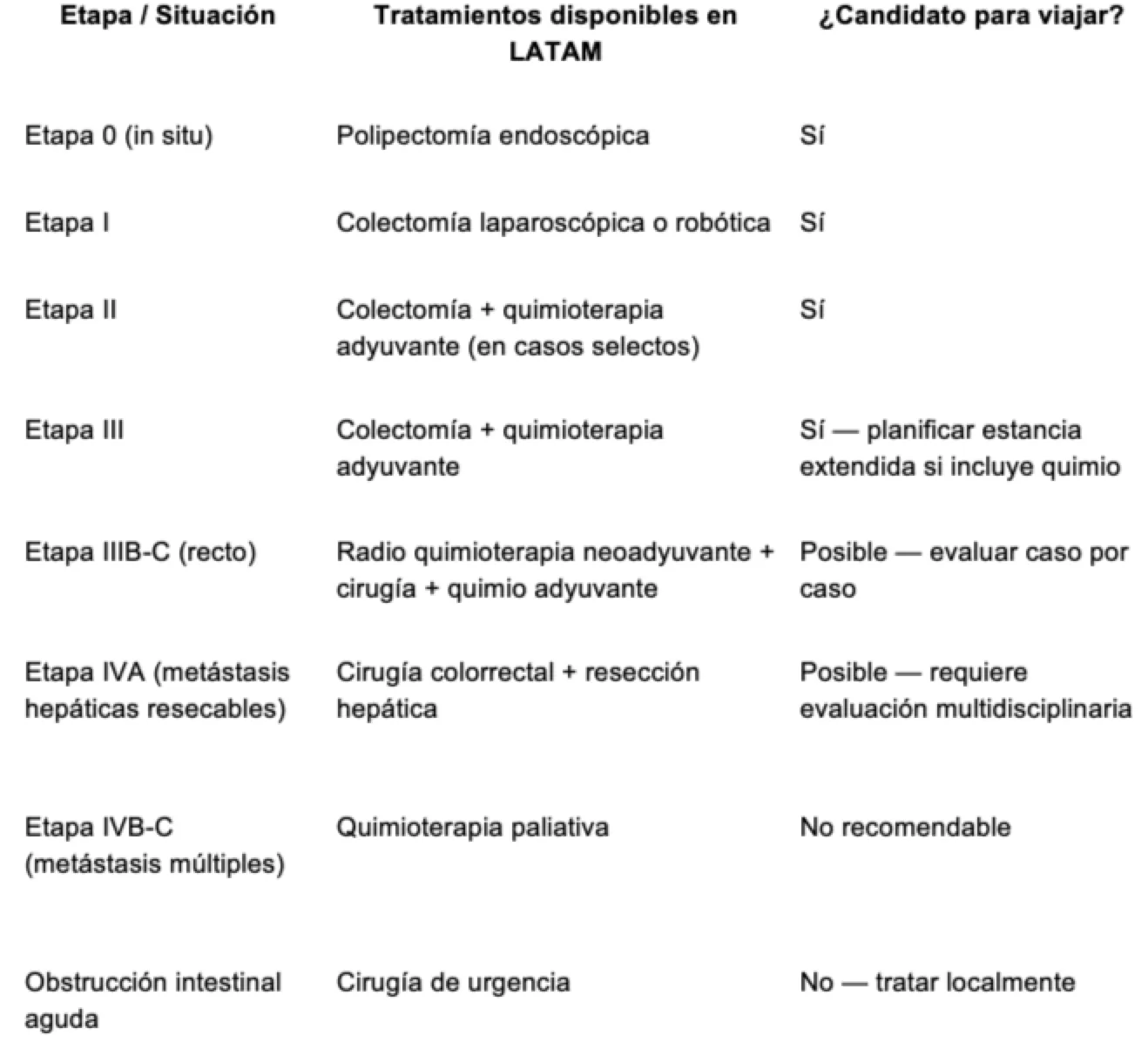
When is it NOT advisable to travel for colorectal cancer treatment?
Your safety always takes precedence over any financial savings. We advise you NOT to consider treatment abroad if you find yourself in any of the following situations:
Advanced metastatic colorectal cancer (stage IVB-C) with extensive peritoneal involvement. These cases require prolonged systemic treatment with close monitoring and the possibility of frequent adjustments. Geographical distance may compromise the continuity of care.
Acute bowel obstruction or perforation. These are surgical emergencies requiring immediate intervention at your nearest hospital. There is no time to plan a journey.
Patients currently undergoing an active neoadjuvant chemotherapy or chemoradiotherapy regimen. Interrupting these treatments can seriously compromise their efficacy. If you have already started a regimen, complete it with your current team and evaluate international options for the subsequent phases.
Uncontrolled active gastrointestinal bleeding. This requires stabilisation and urgent management in your home country.
Severe decompensated comorbidities. Uncontrolled heart, lung, liver or kidney disease significantly increases surgical risk and may contraindicate travel.
At KURBUO, if the surgical oncologist determines during the tele-consultation that your case is not suitable for treatment outside your country, they will inform you directly. We do not compromise your health under any circumstances. We would rather recommend that you seek treatment locally than risk your well-being.
Treatment options for colorectal cancer in Latin America
Leading cancer centres in Colombia and Mexico offer all standard treatment options for colon and rectal cancer, in accordance with the guidelines of the National Comprehensive Cancer Network (NCCN) and the European Society for Medical Oncology (ESMO). Below, we explain each surgical option for colon cancer and the complementary therapies available.
Surgery: Colectomy and tumour resection
Surgery is the main treatment for stage I, II and III colorectal cancer. The aim is to remove the section of the colon or rectum containing the tumour, along with an adequate margin of healthy tissue and the regional lymph nodes, for pathological analysis.
Laparoscopic (minimally invasive) colectomy
This is currently the gold standard for most colon cancers. The surgeon performs the operation through 3–5 small incisions (5–12 mm) using a camera and specialised instruments. The advantages over open surgery are significant: less post-operative pain, faster recovery of bowel function, a shorter hospital stay (3–5 days vs. 7–10 days for open surgery), a lower risk of wound infection, and a quicker return to normal activities.
The oncological outcomes (cure and survival rates) of laparoscopic colectomy are equivalent to those of open surgery, as demonstrated in numerous international studies.
The oncological surgeons at KURBUO in Colombia and Mexico have extensive experience in laparoscopic colorectal surgery and perform this procedure routinely.
Open colectomy
In some cases — such as very large tumours, tumours that have adhered to neighbouring structures, or where there is partial obstruction — open surgery remains the best option. It is performed via a larger incision in the abdomen. Although recovery is slower, it allows the surgeon to have direct control over the surgical field in complex situations.
Robotic surgery for colorectal cancer
Robot-assisted surgery (Da Vinci system) is particularly valuable in rectal cancer, where the surgical space is confined and the preservation of nerves (which control urinary and sexual function) is critical. The magnified 3D view and the millimetre-precise robotic arms allow the surgeon to work with greater control in the deep pelvis.
Colombia and Mexico have centres equipped with Da Vinci systems that perform routine robotic colorectal surgery.
Low anterior resection and ultra-low anterior resection (rectal cancer)
For cancers of the middle and lower rectum, specialised techniques such as low anterior resection (LAR) and ultra-low anterior resection (ULAR) are performed, which aim to remove the tumour whilst preserving the anal sphincter to avoid a permanent colostomy. At KURBUO’s partner centres, these techniques are performed laparoscopically or robotically where the case permits.
In some patients with lower rectal cancer, a temporary colostomy may be necessary during recovery, which is usually reversed in a second operation 2–3 months later. Your surgeon will explain this possibility during the tele-consultation.
Endoscopic polypectomy
For stage 0 cancers (carcinoma in situ) and some very early stage I cases, removal can be performed during a colonoscopy without the need for abdominal surgery. Endoscopy centres in Colombia and Mexico are equipped with high-definition equipment and advanced techniques such as endoscopic submucosal dissection (ESD)
Chemotherapy for colorectal cancer
Chemotherapy is a fundamental component of colorectal cancer treatment, particularly from stage III onwards and in selected stage II cases with high-risk factors.Protocolos estándar disponibles en Latinoamérica:
KURBUO’s partner cancer centres offer all internationally recommended chemotherapy regimens for colorectal cancer:
● FOLFOX (5-fluorouracil + leucovorin + oxaliplatin): The most commonly used adjuvant protocol for stage III. It is generally administered over a period of 3 to 6 months.
● CAPOX / XELOX (capecitabine + oxaliplatin): An oral alternative to FOLFOX, which reduces the need for prolonged intravenous infusions.
● FOLFIRI (5-fluorouracil + leucovorin + irinotecan): Frequently used in advanced disease or as a second-line treatment.
● Oral capecitabine: For patients who are candidates for oral monotherapy.
The medicines used in Colombia and Mexico contain the same active ingredients approved by the FDA. Many are also available as high-quality generics at significantly lower costs.
Terapias biológicas y dirigidas:
Para cáncer colorrectal avanzado o metastásico, están disponibles:
● Bevacizumab (Avastin): Anticuerpo monoclonal anti-VEGF
● Cetuximab (Erbitux): Anticuerpo monoclonal anti-EGFR (para tumores RAS wild-type)
● Panitumumab (Vectibix): Anti-EGFR (para tumores RAS wild-type)
● Pembrolizumab (Keytruda): Inmunoterapia para tumores con alta inestabilidad microsatelital (MSI-H) o deficiencia de reparación de mismatch (dMMR)
Coordination of chemotherapy across countries:
If your treatment plan includes adjuvant chemotherapy following surgery, there are two possible scenarios: completing all cycles in Latin America (requiring a stay of 3–6 months) or having the surgery in Latin America and starting or continuing chemotherapy with your oncologist in the United States. KURBUO coordinates the transfer of treatment protocols, dosages and response data between both medical teams to ensure continuity.
Radiotherapy for colorectal cancer
Dr Esteban Jaramillo states that radiotherapy is mainly used for rectal cancer, not for colon cancer. It plays a particularly important role as a neoadjuvant treatment (before surgery) to reduce the size of the tumour and facilitate a more complete surgical resection.
Modalities available in Latin America:
● Short-course neoadjuvant radiotherapy: 5 sessions over 5 days, followed by surgery the following week. For low- to intermediate-risk rectal cancers.
● Long-course neoadjuvant chemoradiotherapy: 25–28 daily sessions (5–6 weeks) combined with chemotherapy (usually oral capecitabine), followed by surgery 6–8 weeks later. For locally advanced rectal cancers.
● 3D conformal radiotherapy and IMRT: Available at leading cancer centres in Colombia.
If your treatment plan includes neoadjuvant chemoradiotherapy, you should allow for a prolonged stay (8–12 weeks to complete radiotherapy + waiting period + surgery). Your KURBUO specialist will provide you with a detailed schedule during the tele-consultation.
Comparison of colorectal cancer treatment costs: USA vs. Colombia vs. Mexico
The financial impact of colorectal cancer in the United States is devastating. A study published in the Journal of the National Cancer Institute estimated that the average cost of colorectal cancer treatment during the first year after diagnosis exceeds $60,000 for patients with health insurance, and can reach $150,000 or more for those without cover.
For many families, this expense means choosing between their health and their financial stability. It shouldn’t have to be this way.
Comparison table of costs by procedure
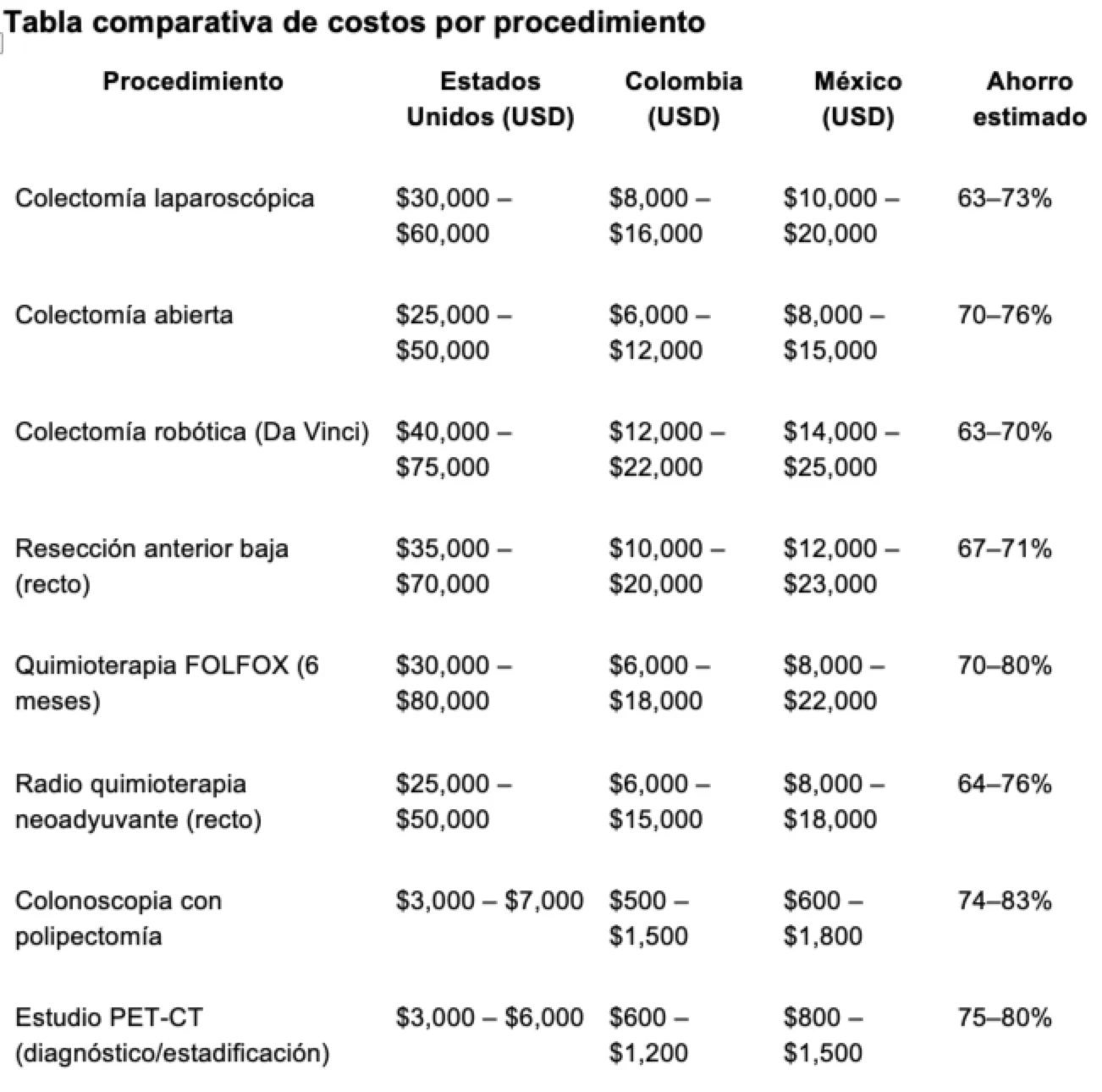
What do these prices include?
Prices for Colombia and Mexico generally include: fees for the surgical oncologist and surgical team, use of the operating theatre (including the robotic system where applicable), post-operative hospital stay (3–7 days depending on the procedure), anaesthesia, pre-operative tests (laboratory tests, imaging, cardiopulmonary and anaesthetic assessments), pathological analysis of the surgical specimen, and post-operative check-ups during your stay.
Prices do not include: international flights, accommodation outside the hospital, post-treatment medication for use at home (painkillers, anticoagulants), nutritional supplements for recovery, or long-term oncological follow-up with your medical team in the United States.
Additional travel expenses
To get a realistic estimate of the total cost of your colorectal cancer treatment in Latin America, take these additional expenses into account: return flights from the US ($300–$600), accommodation during recovery ($50–$150 per night × 10–21 nights depending on the procedure), food and local transport ($30–$60 per day), and travel medical insurance ($150–$400 depending on cover).
Specific example: laparoscopic colectomy
A 55-year-old patient diagnosed with stage II colon cancer who requires a laparoscopic colectomy in the US would face a cost of between $30,000 and $60,000 for the surgery alone. Without insurance, that is the full bill. With insurance, depending on your plan, out-of-pocket expenses can range from $5,000 to $15,000 in co-payments and deductibles.
The same procedure in Colombia — a laparoscopic colectomy performed by a certified oncological surgeon in an accredited hospital — would cost between $8,000 and $16,000. Adding flights ($500), a hotel for 14 nights ($1,400), food and transport ($700), and travel insurance ($300), the total cost would be around $11,000 to $19,000.
Estimated net saving: between $11,000 and $41,000 — including all travel, accommodation and insurance costs.
And if your case only requires a colonoscopy with polypectomy (stage 0 cancer), the savings are even more significant: $500–$1,500 in Colombia compared to $3,000–$7,000 in the US — with no need for hospitalisation or a lengthy recovery.
The prices shown are estimated ranges and may vary depending on the stage of the cancer, the location of the tumour (colon vs. rectum), the surgical technique, and the medical centre. Book your free online consultation with KURBUO to get a personalised estimate based on your specific case.
Is it safe to receive treatment for colorectal cancer in Latin America?
Usted necesita saber dos cosas antes de seguir leyendo: primero, que esta pregunta es completamente válida y cualquier paciente responsable debería hacerla. Segundo, que le vamos a responder con honestidad, no con un discurso de ventas.
Hospitals with specialist oncology units
The treatment of colorectal cancer requires a multidisciplinary approach involving surgical oncologists, medical oncologists, radiotherapists, pathologists, radiologists, gastroenterologists, nutritionists and stoma care specialists (if a stoma is required). Not every hospital can offer this level of coordination.
KURBUO’s partner centres have dedicated oncology units where these multidisciplinary teams work together seamlessly. These hospitals hold tumour boards where specialists from different disciplines review each case together to determine the best treatment plan, exactly as is done in leading cancer centres in the United States.
Accreditations that attest to quality
Joint Commission International (JCI): Colombia has more than 10 hospitals with this accreditation — the same body that certifies leading medical centres in the US. Mexico has a similar number. JCI accreditation assesses more than 1,200 standards relating to patient safety, infection control, medication management and quality of care.
National accreditations: Colombia’s Ministry of Health awards the “Health Accreditation” to institutions that demonstrate sustained excellence. In Mexico, the General Health Council certifies hospitals that meet equivalent standards.
Colorectal oncological surgeons in Latin America
Colorectal surgery is a subspecialty that requires additional training beyond general surgery. KURBUO’s partner colorectal oncological surgeons have specific training in:
● Colorectal cancer surgery using laparoscopic and robotic techniques
● Fellowship at institutions in the United States, Europe or leading centres in Latin America (Hospital Sírio-Libanês in Brazil, the National Cancer Institute in Colombia and Mexico, amongst others)
● Current certification from the national boards of surgical oncology and/or coloproctology
● Membership of societies such as the American Society of Colon and Rectal Surgeons (ASCRS), the Society of Surgical Oncology (SSO) or the European Society of Coloproctology (ESCP)
At KURBUO, every surgeon undergoes a verification process that includes: confirmation of their qualification and subspecialisation, validation of their current certification, verification of their surgical caseload and experience in laparoscopic/robotic colorectal surgery, and a review of their professional background.Tecnología disponible
Leading cancer centres in Colombia are equipped with:
● Da Vinci robotic surgical systems (particularly relevant for rectal surgery)
● High-definition (4K) laparoscopy towers with advanced vascular sealing instruments
● Linear accelerators for 3D conformal radiotherapy and IMRT
● PET-CT and MRI for accurate staging
● Molecular pathology laboratories capable of analysing microsatellite instability (MSI), RAS/BRAF mutations and other biomarkers necessary for defining targeted therapiesManejo de complicaciones
Colorectal surgery carries specific risks, including: anastomotic leakage (leakage at the junction where the ends of the colon are joined), surgical site infection, post-operative ileus (delayed return of bowel function), and bleeding. These risks exist regardless of where the surgery is performed.
Our partner centres are equipped with: intensive care units, surgical teams available 24/7, a blood bank, a laboratory providing results within hours, and ERAS (Enhanced Recovery After Surgery) protocols that speed up recovery and reduce complications.
We strongly recommend taking out travel medical insurance that covers surgical complications.
Coordination with your oncologist at home
Your medical team in the United States will continue to play a vital role in your long-term care. Colorectal cancer requires follow-up with regular colonoscopies, tumour markers (CEA), imaging tests, and possibly adjuvant chemotherapy, which can be administered at home.
Upon completion of your treatment in Latin America, KURBUO facilitates the transfer of your complete medical records to your oncologist in the US, including: a detailed surgical report describing the procedure, histopathology results with pathological staging (pTNM), the number of lymph nodes examined and affected, the status of surgical margins, results of molecular biomarkers (MSI, RAS, BRAF), the chemotherapy protocol administered (if applicable), and diagnostic imaging.
We recommend that you inform your oncologist and gastroenterologist in the US before travelling. Coordination between teams is essential for the continuity of your cancer care.
The step-by-step process with KURBUO for colorectal cancer
The treatment of colorectal cancer can be complex and involve multiple approaches (surgery + chemotherapy + radiotherapy). That is why the process with KURBUO is designed to coordinate everything clearly, step by step, so that you do not have to worry about the medical logistics.

Step 1 — Book your online consultation
Start with a video call with a verified surgical oncologist or coloproctologist, free of charge and with no obligation. You can do this from home, in Spanish or English. Please have your medical documents ready: colonoscopy report with biopsy, pathology results, imaging studies (CT scan, pelvic MRI if rectal cancer, PET-CT if applicable), CEA (carcinoembryonic antigen) levels, and any reports from your current oncologist.
Step 2 — Multidisciplinary assessment of your case
The specialist reviews your full case and determines whether you are a candidate for treatment in Latin America. For colorectal cancer, this assessment is particularly important because the treatment plan may be multimodal. The surgeon assesses: the exact location of the tumour (right colon, transverse colon, left colon, sigmoid colon, rectum), the clinical stage, whether you require neoadjuvant radiotherapy (for rectal cancer), and whether chemotherapy will be administered before, after, or in coordination with your team in the US.
If your case is not suitable, we will inform you with complete transparency. We will not put your health at risk.
Step 3 — Personalised treatment plan and logistics
If you are eligible, you will receive a comprehensive plan: a detailed breakdown of costs by treatment phase (surgery, chemotherapy, radiotherapy — depending on your needs), a schedule with estimated dates and the total length of stay, the medical centre and surgical team assigned to you, guidance on flights, accommodation near the hospital and transport, as well as dietary advice and pre-surgical preparation instructions.
Step 4 — Your treatment
From the moment you arrive, KURBUO coordinates your entire care. You will be met at the airport, provided with bilingual support, and your treatment will take place at the accredited centre you are already familiar with. For a laparoscopic colectomy, the typical hospital stay is 3–5 days. For rectal surgery, it may be 5–7 days. The team maintains constant communication with you and your family.
Step 5 — Post-treatment follow-up and coordination of care continuity
Before you return home, post-operative checks are carried out: verification of bowel function, removal of drains where applicable, wound checks, and confirmation that your recovery is progressing as it should. You will receive a full medical record for your team in the US. If you require adjuvant chemotherapy, KURBUO coordinates the transfer of the treatment plan to your local oncologist, providing all the necessary details to ensure seamless continuity of care.
The tele-consultation is an assessment step. It does not oblige you to travel or commit to any treatment. It is an opportunity to speak with a colorectal cancer specialist, address all your concerns, and gain clarity on your options.
Book your free online consultation with a surgical oncologist
Take the first step — with no obligation
A diagnosis of colorectal cancer requires difficult decisions at a time when you are at your most vulnerable. No one should have to make these decisions without having all the information available, and no one should feel pressured by time or circumstances to make a choice before they are ready.
A tele-consultation with a verified KURBUO surgical oncologist is free, confidential and non-binding. Its aim is simple: to enable you to speak to a specialist, understand your options, and make the decision that is best for your health, your family and your future.
It doesn’t matter whether you decide to move forward today or in a few months’ time. We are here when you are ready.
This guide has been clinically reviewed by the Dr. ESTEBAN JARAMILLO-JIMENEZ, NEURO-ONCOLOGIST, 15 March 2026. This content is for informational purposes only and does not constitute medical advice. Always consult your oncologist or gastroenterologist before making any decisions about your treatment.
Last updated: 17 March 2026





